How accurate are rapid tests, performed during a health-care visit (point-of-care), for diagnosing COVID-19?
Why is this question important?
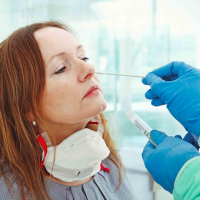
People with suspected COVID-19 need to know quickly whether they are infected, so that they can self-isolate, receive treatment, and inform close contacts. Currently, COVID-19 infection is confirmed by sending away samples, taken from the nose and throat, for laboratory testing. The laboratory test, called RT-PCR, requires specialist equipment, may require repeat healthcare visits, and typically takes at least 24 hours to produce a result.
Rapid point-of-care tests can provide a result ‘while you wait’, ideally within two hours of providing a sample. This could help people isolate early and reduce the spread of infection.
What did we want to find out?
We were interested in two types of rapid point-of-care tests, antigen and molecular tests. Antigen tests identify proteins on the virus, often using disposable devices. Molecular tests detect the virus’s genetic material, using small portable or table-top devices. Both test the same nose or throat samples as RT-PCR tests.
We wanted to know whether rapid point-of-care antigen and molecular tests are accurate enough to replace RT-PCR for diagnosing infection, or to select people for further testing if they have a negative result.
What did we do?
We looked for studies that measured the accuracy of rapid point-of-care tests compared with RT-PCR tests to detect current COVID-19 infection. Studies could assess any rapid antigen or molecular point-of-care test, compared with a reference standard test. The reference standard is the best available method for diagnosing the infection; we considered RT-PCR test results and clinically defined COVID-19 as reference tests. People could be tested in hospital or the community. Studies could test people with or without symptoms.
Tests had to use minimal equipment, be performed safely without risking infection from the sample, and have results available within two hours of the sample being collected. Tests could be used in small laboratories or wherever the patient is (in primary care, urgent care facilities, or in hospital).
How did studies assess diagnostic test accuracy?
Studies tested participants with the rapid point-of-care tests. Participants were classified as known to have – and not to have - COVID-19, by RT-PCR in all studies. Studies then identified false positive and false negative errors in the point-of-care test results, compared to RT-PCR. False positive tests incorrectly identified COVID-19 when it was not present, potentially leading to unnecessary self-isolation and further testing. False negatives missed COVID-19 when it was present, risking delayed self-isolation and treatment, and spread of infection.
What we found
We found 18 relevant studies. Ten studies took place in North America, four in Europe, two in South America, one in China and one in multiple countries.
Nine studies deliberately included a high percentage of people with confirmed COVID-19 or included only people with COVID-19. Fourteen studies did not provide any information about the people providing the samples for testing and 12 did not provide any information about where people were tested.
None of the studies reported included samples from people without symptoms.
Main results
Five studies reported eight evaluations of five different antigen tests. Overall, there was considerable variation between the results of the antigen tests in how well they detected COVID-19 infection. Tests gave false positive results in less than 1% of samples.
Thirteen evaluations of four different molecular tests correctly detected an average of 95% of samples with COVID-19 infection. Around 1% of samples gave false positive results.
If 1000 people had molecular tests, and 100 (10%) of them really had COVID-19:
- 105 people would test positive for COVID-19. Of these, 10 people (10%) would not have COVID-19 (false positive result).
- 895 people would test negative for COVID-19. Of these, 5 people (1%) would actually have COVID-19 (false negative result).
We noted a large difference in COVID-19 detection between the two most commonly evaluated molecular tests.
How reliable were the results of the studies?
Our confidence in the evidence is limited.
- Three-quarters of studies did not follow the test manufacturers’ instructions, so may have found different results if they had.
- Often, studies did not use the most reliable methods or did not report enough information for us to judge their methods. This may have affected estimates of test accuracy, but it is impossible to identify by how much.
- A quarter of studies were published early online as ‘preprints’ and are included in the review. Preprints do not undergo the normal rigorous checks of published studies, so we are uncertain how reliable they are.
What are the implications of this review?
Studies provided little information about their participants, so it is not possible to tell if the results can be applied to people with no symptoms, mild symptoms, or who were hospitalised with COVID-19. Accurate rapid tests would have the potential to select people for RT-PCR testing or to be used where RT-PCR is not available. However, the evidence currently is not strong enough and more studies are urgently needed to be able to say if these tests are good enough to be used in practice.
How up-to-date is this review?
This review includes evidence published up to 25 May 2020. Because new research is being published in this field, we will update this review soon.
- Read the full review on the Cochrane Library
- Visit the Cochrane Infectious Disease Group website
- What are diagnostic test accuracy reviews?
Saturday, September 5, 2020