
Updated systematic review from Cochrane Infectious Diseases Group: Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease.
Updated April 2021: new visual abstract added.
Can symptoms and medical examination accurately diagnose COVID-19?
COVID-19 affects many organs of the body, so people with COVID-19 may have a wide spectrum of symptoms. Symptoms and signs of the illness may be important to help them and the healthcare staff they come into contact with to know whether they have the disease.
Symptoms: people with mild COVID-19 might experience cough, sore throat, high temperature, diarrhoea, headache, muscle or joint pain, fatigue, and loss or disturbance of sense of smell and taste.
Signs are obtained by clinical examination. Signs of COVID-19 examined in this review include lung sounds, blood pressure, blood oxygen level and heart rate.
Often, people with mild symptoms consult their doctor (general practitioner). People with more severe symptoms might visit a hospital outpatient or emergency department. Depending on the results of a clinical examination, patients may be sent home to isolate, may receive further tests or be hospitalised.
Why is accurate diagnosis important?
Accurate diagnosis ensures that people take measures to avoid transmitting the disease and receive appropriate care. This is important for individuals as it reduces harm and it saves time and resources.

نویسندگان قصد فهمیدن چه چیزی را داشتند؟What did the authors want to find out?
The authors wanted to know how accurate diagnosis of COVID-19 is in a primary care or hospital setting, based on symptoms and signs from medical examination.
They searched for studies that assessed the accuracy of symptoms and signs to diagnose COVID-19. Studies had to be conducted in primary care or hospital outpatient settings only. Studies of people in hospital were only included if symptoms and signs were recorded when they were admitted to the hospital.
Lead author of this updated review Thomas Struyf explains,
“The total number of studies included has increased and their overall quality has improved compared to the previous version published in July 2020. We also identified more studies focusing on the diagnostic value of loss of smell or taste.
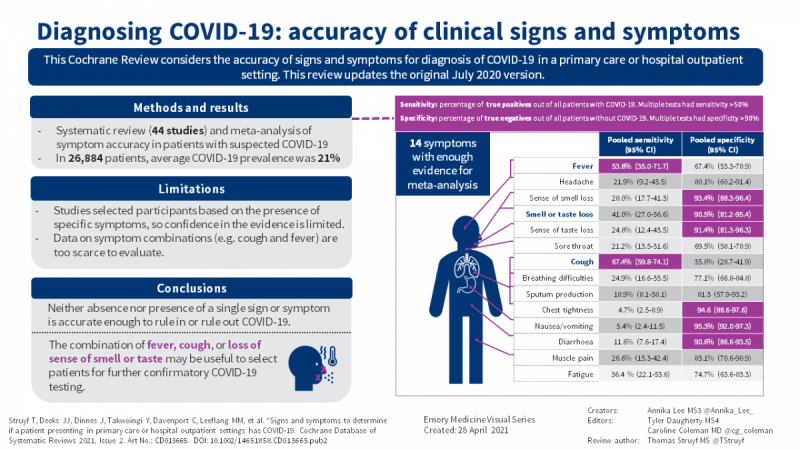
This update confirms that a single symptom or sign cannot accurately diagnose COVID-19. However, the presence of the loss of taste or smell may serve as a red flag for the presence of the disease. The presence of high temperature or cough may also be useful to identify people who might have COVID-19. These symptoms may be useful to prompt further testing when they are present.
We found data on 84 signs and symptoms in 44 studies, but only 10 symptoms were reported by more than 10 studies. So, a lot of these 84 signs and symptoms were not often reported. The top ten most often reported signs and symptoms were fever, cough, shortness of breath, sore throat, muscle soreness, diarrhoea, headache, fatigue, sputum production, and loss of smell or taste.
Importantly our review did not find a lot of studies that investigated combinations of symptoms. Most studies reported a list of individual symptoms, while diagnosis is usually based on a combination of multiple symptoms. We need more evidence on combinations of signs and symptoms before we could recommend an optimal triage-combination.”
The included studies
The authors found 44 relevant studies with 26,884 participants. The studies assessed 84 separate signs and symptoms, and some assessed combinations of signs and symptoms. Three studies were conducted in primary care (1824 participants), nine in specialist COVID-19 testing clinics (10,717 participants), 12 studies in hospital outpatient settings (5061 participants), seven studies in hospitalised patients (1048 participants), 10 studies in the emergency department (3173 participants), and in three studies the setting was not specified (5061 participants). No studies focused specifically on children, and only one focused on older adults.
View this visual abstract is a larger size, download, or print
View this visual abstract in Spanish
Learn more about the Emory medical student visual abstracts
Main results
The studies did not clearly distinguish between mild and severe COVID-19, so the results for mild, moderate and severe disease are presented together.
The symptoms most frequently studied were cough and fever. In our studies, on average 21% of the participants had COVID-19, which means in a group of 1000 people, around 210 would have COVID-19.
According to the studies in our review, in the same 1000 people, around 655 people would have a cough. Of these, 142 would actually have COVID-19. Of the 345 who do not have a cough, 68 would have COVID-19.
In the same 1000 people, around 371 people would have a fever. Of these, 113 would actually have COVID-19. Of the 629 patients without fever, 97 would have COVID-19.
The loss of sense of smell or taste also substantially increase the likelihood of COVID-19 when they are present. For example, in a population where 2% of the people have COVID-19, having either loss of smell or loss of taste would increase a persons’ likelihood of having COVID-19 to 8%.
How reliable are the results?
The accuracy of individual symptoms and signs varied widely across studies. Moreover, the studies selected participants in a way that meant the accuracy of tests based on symptoms and signs may be uncertain.
Conclusions
Most studies were conducted in hospital settings, so the results may not be entirely representative of primary care settings. The results do not apply to children or older adults specifically, and do not clearly differentiate between disease severities.
The results suggest that a single symptom or sign included in this review cannot accurately diagnose COVID-19. However, the presence of loss of taste or smell may serve as a red flag for the presence of the disease. The presence of high temperature or cough may also be useful to identify people who might have COVID-19. These symptoms may be useful to prompt further testing when they are present.
Further research is needed to investigate combinations of symptoms and signs; and testing unselected populations, in primary care settings and in children and older adults.
How up to date is this review?
For this update of the review, the authors searched for studies published from January to July 2020.
- Read the full systematic review
- Read this news item in Chinese and Malay
- Listen to the podcast in English here
- Listen to the podcast in Spanish
- Listen to the podcast in Malay
- Visit the Cochrane Infectious Diseases Group website
- What are diagnostic test accuracy reviews?
- What is the difference between a Cochrane systematic review of interventions and a Cochrane diagnostic test accuracy review?
- Read all the Cochrane resources and news on COVID-19